How are single-site teams different?
Join your peers in the QI enablers study to get us all closer to the answer
The team characteristic data contributed as part of D2D 5.0 show that single-site teams have lower costs, even when patient complexity is considered. This relationship is even stronger than the relationship between quality and cost and was true for both urban and rural teams. It seems to persist over time with improving trends in cost and quality for teams in single sites (see graph below). 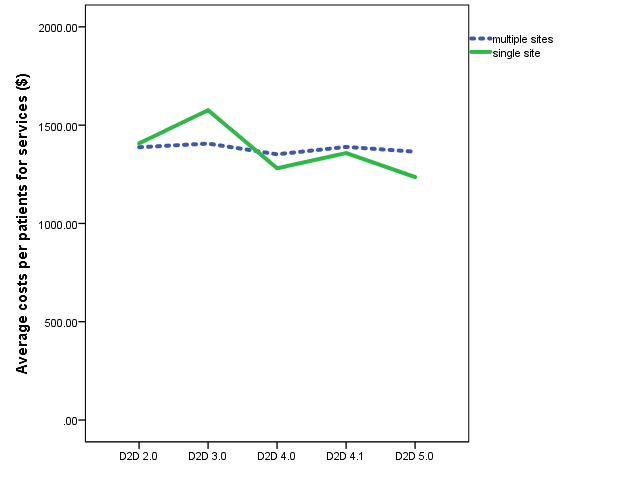 Perhaps surprisingly, there is no relationship with QI activities, conversations with physicians or physician champions, suggesting that these activities might not be driving the changes in costs and quality. So the question remains: How are single-site teams different? The question is part of the QI enablers study, already underway with a half-dozen members (for whose participation we are very thankful!). As part of this study, AFHTO staff are looking to talk to a few more single-site teams as well as some multiple-site teams to learn about similarities and differences. Here are some of the questions we want to dig into:
Perhaps surprisingly, there is no relationship with QI activities, conversations with physicians or physician champions, suggesting that these activities might not be driving the changes in costs and quality. So the question remains: How are single-site teams different? The question is part of the QI enablers study, already underway with a half-dozen members (for whose participation we are very thankful!). As part of this study, AFHTO staff are looking to talk to a few more single-site teams as well as some multiple-site teams to learn about similarities and differences. Here are some of the questions we want to dig into:
- Does single-site mean co-location of IHPs and physicians? This is one of factors thought to be associated with the positive impact of teams.
- What unique aspects of single-site teams (besides the obvious physical structure) should or could be tried in multiple-site teams to help them achieve similar improvements in cost and quality?
Only AFHTO members can answer these questions because only AFHTO members had the vision, courage and conviction to share the necessary data to support these analyses. In this way, AFHTO members are best equipped to tell the stories to demonstrate their own value. If you would like to join your peers in this important process, please let carol.mulder@afhto.ca know when you might be available for a telephone interview to help us all get closer to the answer.